Increased Safety for Elevator Doors
Apr 2, 2024

This paper was presented at the 2022 International Elevator & Escalator Symposium in Barcelona, Spain.
ABSTRACT
In North America, various studies have shown that elevator door strikes continue to be a hazard for elevator users. Consequently, the North American standard for elevators, ANSI A17.1-2019/ CSA B44-19, now includes new protection requirements for increased safety. Besides the common method of a two-dimensional protective field generated by a light curtain, the standard describes new requirements to detect approaching passengers.
CEDES investigated different technologies and checked which of these are suitable to fulfill the new 3D requirements, including:
- 3D light curtains
- Radar sensors
- Cameras
3D light curtains are installed between the car doors and the hoistway doors. Some portion of their field of view is often obstructed by a leading hoistway door, rendering them an impractical solution to fulfill the required detection field.
Radar sensors can be installed on the transom of the elevator opening, but the sensitivity of those sensors is difficult to control. The field of sensitivity is easily much too large so that objects in too large of distances are recognized. And most importantly, U.S. standards require a minimum distance between radar sensors and humans, which cannot be guaranteed in an elevator.
Time of flight (ToF) camera systems provide a reliable integrated distance measurement to detect approaching passengers and to distinguish those from closing doors. It is also possible to pack this technology in an acceptable form factor that allows the camera to be flush mounted and still fit in most transoms. ToF technology was, therefore, clearly the best solution.
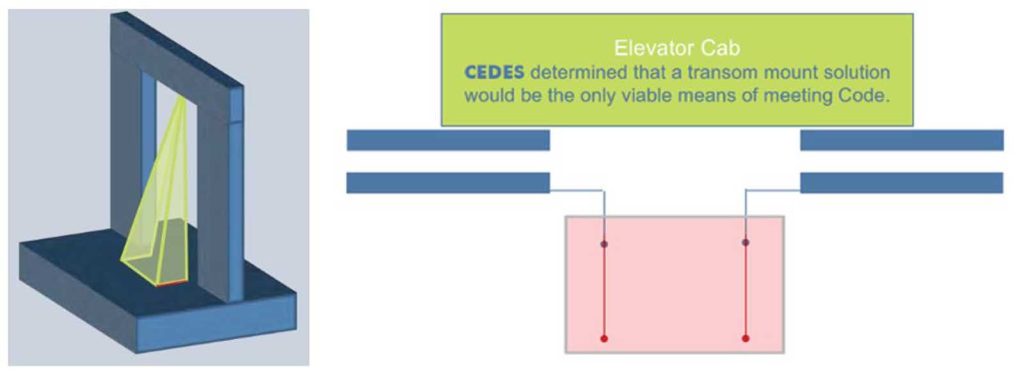
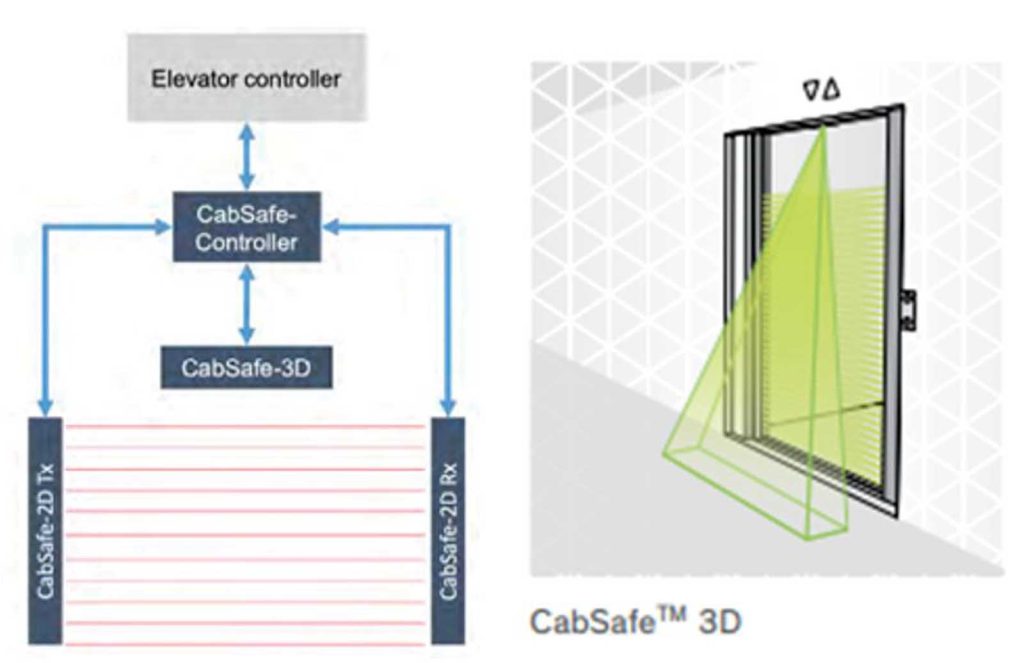
The CEDES CabSafe system, a ToF-camera system supports left-, right- and center-opening applications, regardless of door panel thickness or gap between the doors, or when the landing door leads the cab door during the closing cycle. The CabSafe system is third-party tested to fulfill the 2019 elevator safety code.
PAPER
When elevators became commercially feasible, building owners utilized elevator attendants (people) to actually run each individual elevator and ensure that elevator doors did not close on passengers or objects entering the elevator cab. Over time, however, technology started to replace what had become known as “attended operation,” primarily due to the expense of needing personnel available to run many elevators seven days a week, some with 24-h operation.
Relative to door protection, one of the first technologies used was the mechanical safety edge — sometimes referred to as door bumpers or door buffers. These devices are attached to moving elevator cab doors, and when they come in contact with a person or object, are depressed, causing the change of state of an associated electrical contact that, in turn, generates a reopen signal back to the elevator control. Mechanical safety edges generally cover the full door opening but require contact with the person or object in order to cause this reopen signal to be generated (i.e., a person or object must be “hit” by the mechanical safety edge).
To address this “contact” requirement, several elevator manufacturers used the mechanical safety edge with one or two single beam photoelectric sensors added to the safety circuit. In fact, CEDES was born in 1986 when the founder was asked to develop this single beam solution for a major elevator manufacturer. These photoelectric sensors were located on the elevator cab near or on the cab door(s) and were used to detect the presence of a leg or body in the opening so that detection could occur prior to impact by the mechanical safety edge. In this configuration, there are still only one or two points of non-contact detection and, hence, other body parts (e.g., head) could still be “hit” by the mechanical safety edge.
This progressed to using a light curtain — a device where many photoelectric sensors are mounted in a single housing and operate as a single system. A light curtain is still mounted on the elevator cab door(s) but replaces the mechanical safety edge and is a completely non-contact solution because the detection means does not require a person or object to make contact with the device to generate the reopening signal. When one or more of the light beams become interrupted, the door reopen signal is automatically generated. Over the years, this solution has become the de facto standard for elevators in North America.
All of these solutions fulfill the requirements defined in Section 2.13.5 of ANSI A17.1-2016/CSA B44-16, the Safety Code for Elevators and Escalators (the “Code”), as well as earlier versions of the Code. The 2016 Code, and previous versions, basically require that when a “reopening device” is used in power-operated horizontally sliding car door applications, it must be effective for “substantially the full vertical opening of the door.”[1]
But injury data suggests that improvements are still needed to reduce the number of injuries that continue to occur during elevator door closing.
Three studies were performed by the Department of Public Health at the Indiana University School of Medicine that provide detail on injuries still occurring in passenger elevator applications. All studies utilized the U.S. Consumer Product Safety Commission (CPSC) National Electronic Injury Surveillance System (NEISS),[2] a database that provides injury statistics based on emergency room visits at one of 100 NEISS-designated hospitals.
The NEISS database does not include injuries that result in death or injuries that are only treated at the scene of an incident. It only includes injuries associated with emergency room visits and, hence, it is likely that the total number of incidents that occurred in the referenced time frames below are actually underreported.
- For children from 0 to 19 years of age, NEISS data indicated that, statistically, 18,750 elevator injuries (64.5%) were due to an elevator door closing on a body part of the 29,030 total injuries estimated to have occurred between 1990 and 2004 (O’Neill, et. Al., 2007).[3]
- For adults from 20 to 64 years old, NEISS data indicated that, statistically, 23,659 elevator injuries (42.5%) were due to an elevator door closing on a body part of the 55,614 total injuries estimated to have occurred between 1990 and 2002 (Morrison-Ibrahim, Between 2010-2012).[4]
- For adults 65 years old and older, NEISS data indicated that, statistically, 15,166 elevator injuries (33.8%) were due to an elevator door closing on a body part or walker wedged in the door of the 44,870 total injuries estimated to have occurred between 1990 and 2006 (Steele, et. Al., 2010).[5]
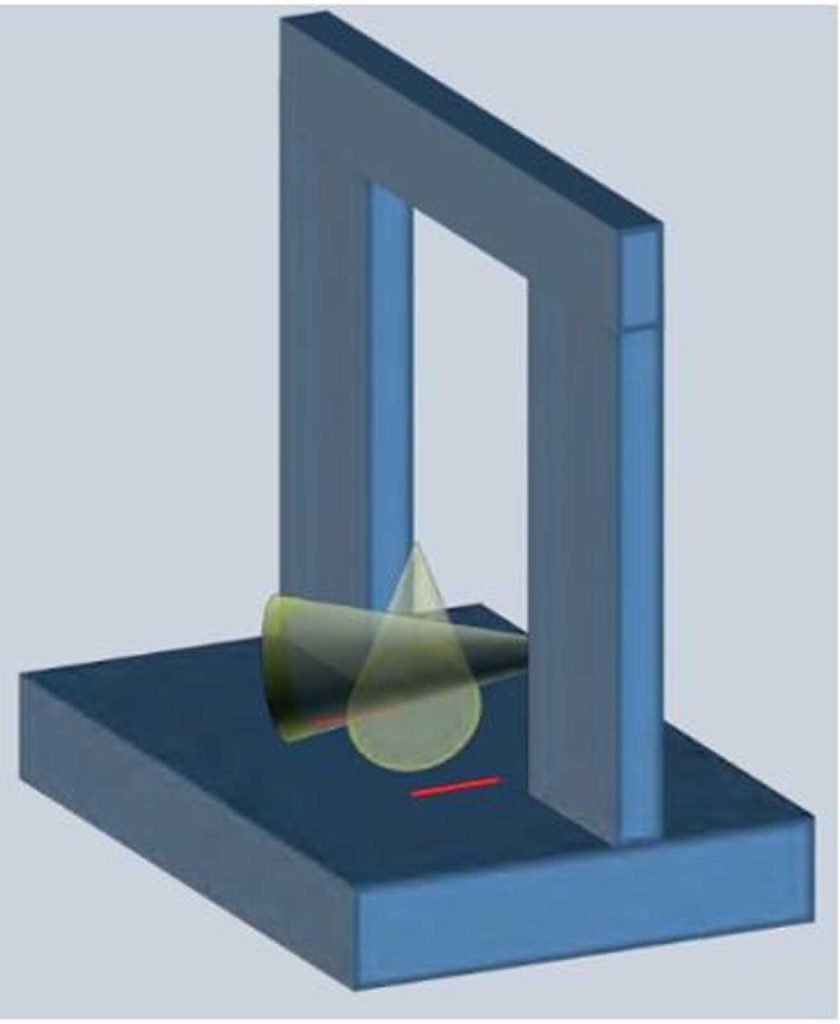
Using this data, the number of emergency room visits attributed to an elevator door(s) closing on a body part or a walker being wedged in the elevator door(s) is nearly 4,000 annually, and additional hazards, such as the leading edge of the landing side of the landing door, still need to be addressed (see Figure 1).




Get more of Elevator World. Sign up for our free e-newsletter.
![]()








![]()